Sending Updates Through The Provider Healthcare Portal. Indiana Health Coverage Programs DXC Technology October 2017
|
|
|
- Julianna West
- 6 years ago
- Views:
Transcription

1 Sending Updates Through The Provider Healthcare Portal Indiana Health Coverage Programs DXC Technology October 2017
2 Agenda Features of Electronic Enrollment Updates and Reminders Provider Maintenance Navigation Updates that can be made on the Portal Revalidation and Recertification Helpful Tools Questions 2
3 Features of Electronic Enrollment Updates and Reminders 3
4 Features of Electronic Enrollment Updates Faster and more convenient than mailing paper applications or forms Transmissions can be saved and returned to later for submission Personal information is secure Required supporting enrollment documentation attachments can be directly uploaded for submission Real-time status of some submitted updates Some updates made on the Portal are immediate 4
5 Immediate Changes Contact and Delegate Administrator changes Address changes (other than Home address) Specialty changes that do not require documentation Presumptive Eligibility election EFT add (18 day paper check during change period) EFT deletion Language 590 and MRT election Rendering Provider Termination Taxonomy removal Medicare participation 5

6 Reminder Providers are reminded that the Provider Agreement states updates and changes to the provider enrollment information are to be reported within 30 days of the change Medicare and Medicaid compare enrollment data Differences in reported information can cause audits to occur 6
7 Provider Maintenance Portal Navigation 7

8 Need to Know Review instructions and information provided on each page before submission When viewing only, no changes are made Changes are electronically submitted to DXC when clicking Submit The following confirmation window appears when clicking Cancel 8
9 Electronic Attachments Any changes that require documentation trigger the attachment screen 9

10 Attachments by Mail Attachments are able to be sent by mail also 10
11 Updates that can be made on the Provider Healthcare Portal 11

12 12 Provider Maintenance

13 13 Update Options Available

14 14 Change Tax ID

15 Contact and Delegated Administrator Changes Person who can answer questions regarding the location 15

16 16 Delegated Administrator Changes

17 17 Address Changes

18 18 Specialty Changes
19 19 Presumptive Eligibility

20 20 Electronic Funds Transfer

21 21 Language Changes

22 Electronic Remittance Advice Changes Can Cancel or Change ERA 22

23 23 Other Information Changes

24 24 Other Information Changes
25 Rendering Provider Changes - Add 25 Click Add and Submit
26 26 Rendering Provider Changes Attachments


27 27 Rendering Provider Changes - Remove
28 Provider Identification Changes Changes that fall under this category: Provider Legal Name Organizational Structure Provider Identification (NPI) Taxonomy Information License Information Medicare Participation Patient Population CLIA Certification DEA Number 28

29 29 Provider Identification Changes

30 30 Provider Identification Changes

31 Provider Identification Changes Include all taxonomy codes that reflect the services provided at the location. 31
32 Provider Identification Changes 32 When Recertifying - use this screen and attach required documents

33 33 Provider Identification Changes

34 Provider Identification Changes Attachment is required 34

35 Disclosure Changes Managing Individuals 35

36 36 Disclosure Changes
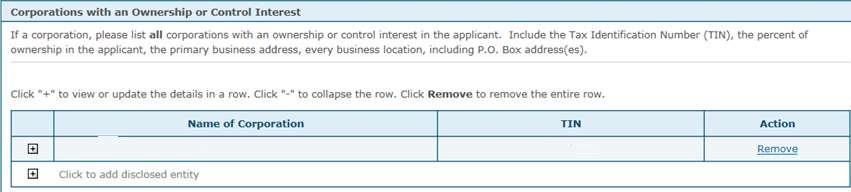
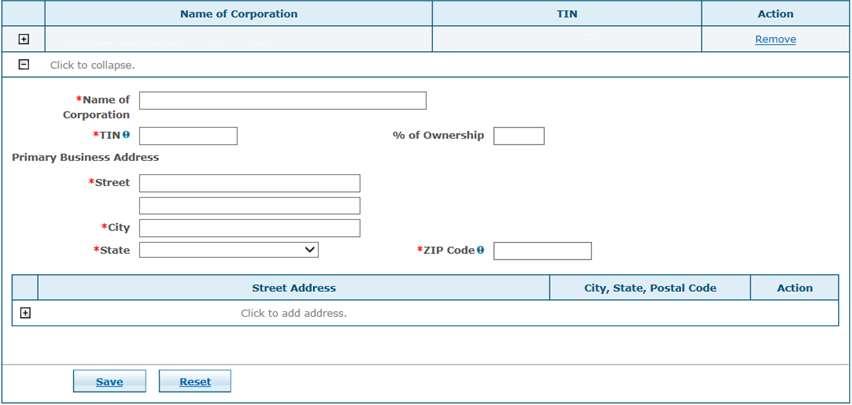
37 37 Disclosure Changes

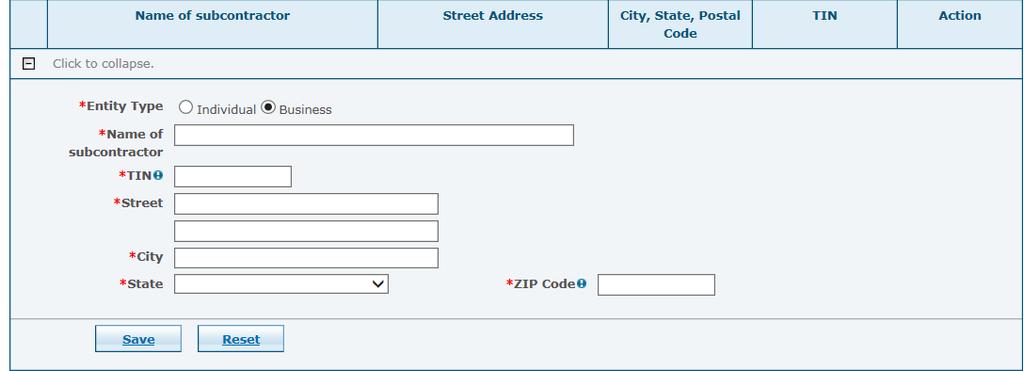
38 38 Disclosure Changes

39 39 Tracking Number
40 Checking Change Request Status After transaction is submitted, the status of the transaction can be checked any time in the Portal, without calling Customer Service. IMPORTANT: For security reasons, the application tracking number (ATN), password, and the federal taxpayer identification number (TIN) or employer identification number (EIN) are required to view the submitted transaction status 40

41 41 Pending Updates

42 42 Check Status


43 Return to Provider Additional Information Requests If information is missing or inaccurate on an electronic submission, you have 21 days to correct and resubmit the transaction. Contact listed on application will receive notification Notification will be sent to the Mail To address listed on application or group location Follow instructions on letter and resubmit 43
44 Check Status Status Code and Description What does it mean? A-Approved The enrollment transaction request has been approved F-Completed D-Denied The enrollment transaction maintenance task has been completed. The enrollment application has been denied. This status also appears when an RTP as not been returned and has expired (21-days old). I-Incomplete W-Provider Corrections Required K-Ready For Review The enrollment transaction request has been denied or had inaccurate or missing information which was not corrected in the 21-day timeframe. The enrollment transaction has been partially completed by the user and saved but not yet submitted The transaction has missing or inaccurate information and must be corrected and resubmitted within 21 days. The enrollment transaction was received but has not yet entered the review process due to date of receipt, pending attachments sent by mail, or an error. S-Resubmit Application The corrected enrollment transaction has been received timely but has not yet entered into the review process. L-Under 44 Review The enrollment transaction or maintenance task is currently being reviewed.
45 45 Revalidation and Recertification

46 Revalidation Revalidation letters are sent to the MAIL TO address 60 and 90 days prior to the revalidation due date Yellow triangle appears under the Provider portion of the Home Page Notifies of revalidation due for that particular location Check status from the service location account Revalidation application is prepopulated with provider service location information Rendering provider agreements are REQUIRED for electronic and paper revalidation TO PREVENT CLOSURE OF THE SERVICE LOCATION FOR FAILURE TO REVALIDATE, SUBMIT THE REVALIDATION AS SOON AS THE FIRST NOTIFICATION IS RECEIVED. 46


47 Revalidation Choose the Re-Validation link on the left side of the My Home page. 47
48 Recertification Certain provider types are required to recertify by updating expiring licenses, insurance information, and certifications (as applicable) with the IHCP. Provider type 01 - Hospitals that are out of state (OOS) Provider type 26 - Transportation providers of all specialties Provider type 28 - Out-of-state Laboratory providers with Specialty Mobile Lab or Mobile Independent Diagnostic Testing Facility (IDTF) Provider type 29 - Out-of-state Radiology providers with Specialty Mobile X-Ray Clinic. Notification is sent to the provider Mail To address 60 business days before the end date of the provider's eligibility to participate Failure to recertify timely will require a full re-enrollment with the IHCP 48
49 Provider Identification Changes When Recertifying - use this screen and attach required documents 49
50 50 Helpful Tools

51 Helpful Tools IHCP website at indianamedicaid.com IHCP Provider Reference Modules Medical Policy Manual Customer Assistance available 8am-6pm EST Monday Friday IHCP Provider Relations Field Consultants See the Provider Relations Field Consultants page at indianamedicaid.com Secure Correspondence via the Provider Healthcare Portal Written Correspondence DXC Technology Provider Written Correspondence P.O. Box 7263 Indianapolis, In
52 52 Questions Following this session please review your schedule for the next session you are registered to attend
Provider Healthcare Portal
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Provider Healthcare Portal L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 5 9 P U B L I S H E D : F E B R U A R Y 1 6, 2 0 1
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Provider Healthcare Portal L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 5 9 P U B L I S H E D : F E B R U A R Y 1 6, 2 0 1
Rhode Island Medicaid Provider Enrollment User Guide. Executive Office of Health and Human Services Medicaid
 Rhode Island Executive Office of Health and Human Services Medicaid Ordering, Prescribing, Referring Provider User Guide Version 1.0 DXC Technology PR0123 V1.0 06/19/2017 Rhode Island Page 1 of 24 Revision
Rhode Island Executive Office of Health and Human Services Medicaid Ordering, Prescribing, Referring Provider User Guide Version 1.0 DXC Technology PR0123 V1.0 06/19/2017 Rhode Island Page 1 of 24 Revision
Provider Healthcare Portal Registration FAQs
 Registration FAQs These are some of the questions the Indiana Health Coverage Programs (IHCP) is asked most frequently about registering for the new (Portal). For detailed information on registering for
Registration FAQs These are some of the questions the Indiana Health Coverage Programs (IHCP) is asked most frequently about registering for the new (Portal). For detailed information on registering for
B I L L I N G P R O V I D E R U P D A T E F O R M I N S T R U C T I O N S ( F O R G R O U P S, F A C I L I T I E S, A N D S O L E
 Indiana Health Coverage Programs General Instructions Please read carefully B I L L I N G P R O V I D E R U P D A T E F O R M I N S T R U C T I O N S ( F O R G R O U P S, F A C I L I T I E S, A N D S O
Indiana Health Coverage Programs General Instructions Please read carefully B I L L I N G P R O V I D E R U P D A T E F O R M I N S T R U C T I O N S ( F O R G R O U P S, F A C I L I T I E S, A N D S O
Connecticut Medical Assistance Program Enrollment Wizard. Presented by The Department of Social Services & HP Enterprise Services 1
 Connecticut Medical Assistance Program Enrollment Wizard Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics www.ctdssmap.com Enrollment Wizard Connecticut Medical
Connecticut Medical Assistance Program Enrollment Wizard Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics www.ctdssmap.com Enrollment Wizard Connecticut Medical
Welcome to ProviderNet. ProviderNet Molina Registration Instructions Revised: January 2015
 Welcome to ProviderNet ProviderNet Molina Registration Instructions Revised: January 2015 1 Introduction Alegeus Technologies is pleased to provide the following registration instructions for the ProviderNet
Welcome to ProviderNet ProviderNet Molina Registration Instructions Revised: January 2015 1 Introduction Alegeus Technologies is pleased to provide the following registration instructions for the ProviderNet
Connecticut Medical Assistance Program Enrollment Workshop for Connecticut Home Care (CHC) Service Providers
 Service Providers") Connecticut Medical Assistance Program Enrollment Workshop for Connecticut Home Care (CHC) Service Providers Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Program
Connecticut Medical Assistance Program Enrollment Workshop for Connecticut Home Care (CHC) Service Providers Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Program
Interactive Voice Response System
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Interactive Voice Response System L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 0 2 P U B L I S H E D : J A N U A R Y 1 1,
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Interactive Voice Response System L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 0 2 P U B L I S H E D : J A N U A R Y 1 1,
Group Provider Enrollment Tutorial. Revised 4/5/18
 Group Provider Enrollment Tutorial Revised 4/5/18 1 Group Provider Enrollment Documents you will need: Copy of Confirmation Letter or email from the National Plan and Provider Enumeration System (NPPES)
Group Provider Enrollment Tutorial Revised 4/5/18 1 Group Provider Enrollment Documents you will need: Copy of Confirmation Letter or email from the National Plan and Provider Enumeration System (NPPES)
CAQH ProView. Dentist Practice Manager Module User Guide
 CAQH ProView Dentist Practice Manager Module User Guide Table of Contents Chapter 1: Introduction... 1 CAQH ProView Overview... 1 System Security... 2 Chapter 2: Registration... 3 Existing Practice Managers...
CAQH ProView Dentist Practice Manager Module User Guide Table of Contents Chapter 1: Introduction... 1 CAQH ProView Overview... 1 System Security... 2 Chapter 2: Registration... 3 Existing Practice Managers...
220 Burnham Street South Windsor, CT Vox Fax
 220 Burnham Street South Windsor, CT 06074 Vox 888-255-7293 Fax 860-289-0055 DELTA DENTAL OF WISCONSIN DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 39069 SPECIAL NOTES
220 Burnham Street South Windsor, CT 06074 Vox 888-255-7293 Fax 860-289-0055 DELTA DENTAL OF WISCONSIN DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 39069 SPECIAL NOTES
Data Type and Format (Not all data elements require a format specification)
") Individual Data Element Name (Term) Sub-element Name (Term) Data Element Description Data Type and Format (Not all data elements require a format specification) Data Element Requirement for Health Plan
Individual Data Element Name (Term) Sub-element Name (Term) Data Element Description Data Type and Format (Not all data elements require a format specification) Data Element Requirement for Health Plan
ERA Enrollment Form Enrolling Through emomed
 ERA Enrollment Rule 382 requires an electronic option for providers and trading partners to complete and submit the ERA enrollment effective January 1, 2014. An online ERA enrollment link from the emomed
ERA Enrollment Rule 382 requires an electronic option for providers and trading partners to complete and submit the ERA enrollment effective January 1, 2014. An online ERA enrollment link from the emomed
BCBS LOUISIANA PRE-ENROLLMENT INSTRUCTIONS 53120
 BCBS LOUISIANA PRE-ENROLLMENT INSTRUCTIONS 53120 HOW LONG DOES PRE-ENROLLMENT TAKE? Standard Processing time is 3 business days WHAT FORM(S) DO I COMPLETE? BCBS LA EDI Transaction Addendum Business Associate
BCBS LOUISIANA PRE-ENROLLMENT INSTRUCTIONS 53120 HOW LONG DOES PRE-ENROLLMENT TAKE? Standard Processing time is 3 business days WHAT FORM(S) DO I COMPLETE? BCBS LA EDI Transaction Addendum Business Associate
Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
Claim Settings Guide May 2012
 Claim Settings Guide May 2012 Kareo Claim Settings Guide April 2012 1 Table of Contents 1. INTRODUCTION... 1 2. CONFIGURE PRACTICE SETTINGS... 2 3. CONFIGURE PROVIDER CLAIM SETTINGS... 4 3.1 Enter General
Claim Settings Guide May 2012 Kareo Claim Settings Guide April 2012 1 Table of Contents 1. INTRODUCTION... 1 2. CONFIGURE PRACTICE SETTINGS... 2 3. CONFIGURE PROVIDER CLAIM SETTINGS... 4 3.1 Enter General
Guide to Completing the Electronic Remittance Advice (ERA) Enrollment Form
 Enrollment Form") Guide to Completing the Electronic Remittance Advice (ERA) Enrollment Form The ERA service enables Blue Cross and Blue Shield of Louisiana to provide you with an electronic remittance advice, which is
Guide to Completing the Electronic Remittance Advice (ERA) Enrollment Form The ERA service enables Blue Cross and Blue Shield of Louisiana to provide you with an electronic remittance advice, which is
MASSACHUSETTS BCBS SB700 SUBMITTER ID - U076 12B14 SUBMITTER ID 00444PVRM
 MASSACHUSETTS BCBS SB700 SUBMITTER ID - U076 12B14 SUBMITTER ID 00444PVRM https://provider.bluecrossma.com/providerhome/portal/home/forms/forms/era Instructions for Completing BCBSMA Electronic Remittance
MASSACHUSETTS BCBS SB700 SUBMITTER ID - U076 12B14 SUBMITTER ID 00444PVRM https://provider.bluecrossma.com/providerhome/portal/home/forms/forms/era Instructions for Completing BCBSMA Electronic Remittance
220 Burnham Street South Windsor, CT Vox Fax
 DELTA DENTAL OF ILLINOIS GROUP PLANS DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 05030 SPECIAL NOTES Participation with Direct Deposit (EFT) is required for receipt
DELTA DENTAL OF ILLINOIS GROUP PLANS DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 05030 SPECIAL NOTES Participation with Direct Deposit (EFT) is required for receipt
CORE-required Maximum EFT Enrollment Data Set
 CORE-required Maximum EFT Data Set The following table is taken directly from CORE Operating Rule 380 and identifies all details related to the fields contained within this document. Individual Data Element
CORE-required Maximum EFT Data Set The following table is taken directly from CORE Operating Rule 380 and identifies all details related to the fields contained within this document. Individual Data Element
Authorization Agreement
 Authorization Agreement For Electronic Health Care Claim Payment / Advice 835 Thank you for your interest in the Electronic Health Care Claim Payment/Advice (835), also known as Electronic Remittance Advice
Authorization Agreement For Electronic Health Care Claim Payment / Advice 835 Thank you for your interest in the Electronic Health Care Claim Payment/Advice (835), also known as Electronic Remittance Advice
220 Burnham Street South Windsor, CT Vox Fax
 NEVADA MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CKNV1 Participation in Dental Electronic Remittance Advice
NEVADA MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CKNV1 Participation in Dental Electronic Remittance Advice
Louisiana Medicaid Management Information System (LMMIS)
") Louisiana Medicaid Management Information System (LMMIS) EFT Authorization Application User Guide Date Created: 1/23/2014 Date Revised: 8/03/2018 Prepared By Technical Communications Group Molina Medicaid
Louisiana Medicaid Management Information System (LMMIS) EFT Authorization Application User Guide Date Created: 1/23/2014 Date Revised: 8/03/2018 Prepared By Technical Communications Group Molina Medicaid
Provider Portal User Guide
 Provider Portal User Guide Updated: January 1, 2019 Table of Contents Introduction... 1 How to Register for the Provider Portal... 3 Manage Your Profile... 5 User Administration... 8 Authorizations & Referrals...
Provider Portal User Guide Updated: January 1, 2019 Table of Contents Introduction... 1 How to Register for the Provider Portal... 3 Manage Your Profile... 5 User Administration... 8 Authorizations & Referrals...
Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
Provider Information Management System (PIMS) User Guide
 User Guide") Provider Information Management System (PIMS) User Guide v2018_0807 Overview The Provider Information Management System (PIMS) application is used to manage and maintain provider accounts. It is accessed
Provider Information Management System (PIMS) User Guide v2018_0807 Overview The Provider Information Management System (PIMS) application is used to manage and maintain provider accounts. It is accessed
220 Burnham Street South Windsor, CT Vox Fax
 220 Burnham Street South Windsor, CT 06074 Vox 888-255-7293 Fax 860-289-0055 DELTA DENTAL OF ILLINOIS GROUP PLANS DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 05030
220 Burnham Street South Windsor, CT 06074 Vox 888-255-7293 Fax 860-289-0055 DELTA DENTAL OF ILLINOIS GROUP PLANS DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 05030
Louisiana Medicaid Management Information System (LMMIS)
") Louisiana Medicaid Management Information System (LMMIS) Electronic 835 Remittance Advice (ERA) Authorization Agreement Application User Manual Date Created: 08/06/2018 Date Modified: 12/03/2018 Prepared
Louisiana Medicaid Management Information System (LMMIS) Electronic 835 Remittance Advice (ERA) Authorization Agreement Application User Manual Date Created: 08/06/2018 Date Modified: 12/03/2018 Prepared
2777 Stemmons Frwy, Suite 1450 Dallas, TX Fax
 Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
District of Columbia Department of Health Care Finance. Provider Data Management System and Service (PDMS) Project
 Project") District of Columbia Department of Health Care Finance Provider Data Management System and Service (PDMS) Project How to Enroll in DC Medicaid Using the DC Provider Screening and Enrollment Web Portal
District of Columbia Department of Health Care Finance Provider Data Management System and Service (PDMS) Project How to Enroll in DC Medicaid Using the DC Provider Screening and Enrollment Web Portal
220 Burnham Street South Windsor, CT Vox Fax
 NEW HAMPSHIRE MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER SPECIAL NOTES CKNH1 ERAs can only be sent to one Trading Partner, if a provider has previously requested
NEW HAMPSHIRE MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER SPECIAL NOTES CKNH1 ERAs can only be sent to one Trading Partner, if a provider has previously requested
EDI-ERA Provider Agreement and Enrollment Form (Page 1 of 5)
") (Page 1 of 5) Please complete the following Mississippi Medicaid EDI ERA Provider Agreement and Enrollment Form. Please print or type. Complete all areas of the form, unless otherwise indicated. Once the
(Page 1 of 5) Please complete the following Mississippi Medicaid EDI ERA Provider Agreement and Enrollment Form. Please print or type. Complete all areas of the form, unless otherwise indicated. Once the
Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
Medicare Advantage Provider Resource Guide
 Medicare Advantage Provider Resource Guide Thank you for being a star member of our provider team. WellCare Health Plans, Inc., (WellCare) understands that having access to the right tools can help you
Medicare Advantage Provider Resource Guide Thank you for being a star member of our provider team. WellCare Health Plans, Inc., (WellCare) understands that having access to the right tools can help you
TRICARE PGBA, LLC Electronic Data Interchange PO Box Augusta, GA Fax: Phone , Option #2
 TRICARE PGBA, LLC Fax: 803-264-9864 Phone 1-800-325-5920, Option #2 Dear Provider: Thank you for your interest in Electronic Remittance Advice (ERA) with PGBA, LLC. We also offer Electronic Funds Transfer
TRICARE PGBA, LLC Fax: 803-264-9864 Phone 1-800-325-5920, Option #2 Dear Provider: Thank you for your interest in Electronic Remittance Advice (ERA) with PGBA, LLC. We also offer Electronic Funds Transfer
TRICARE West Region Electronic Data Interchange PO Box Augusta, GA Fax:
 Dear Provider: Thank you for your interest in Electronic Remittance Advice (ERA) with PGBA, LLC. Please take a moment to review the enrollment guidelines (Appendix A). Once you have reviewed the guidelines,
Dear Provider: Thank you for your interest in Electronic Remittance Advice (ERA) with PGBA, LLC. Please take a moment to review the enrollment guidelines (Appendix A). Once you have reviewed the guidelines,
220 Burnham Street South Windsor, CT Vox Fax
 NEBRASKA MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER SPECIAL NOTES CKNE1 Paper Remittance Advice Statements and Refund Request Reports statements will cease
NEBRASKA MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER SPECIAL NOTES CKNE1 Paper Remittance Advice Statements and Refund Request Reports statements will cease
Change Healthcare CLAIMS Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare CLAIMS Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider
PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare CLAIMS Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider
BCBS LOUISIANA (53120) PRE-ENROLLMENT INSTRUCTIONS
 PRE-ENROLLMENT INSTRUCTIONS") BCBS LOUISIANA (53120) PRE-ENROLLMENT INSTRUCTIONS WHAT FORM(S) SHOULD I DO? BCBS LA Business Associate Profile Electronic Remittance Advice (ERA) Enrollment form If you would like to receive ERAs through
BCBS LOUISIANA (53120) PRE-ENROLLMENT INSTRUCTIONS WHAT FORM(S) SHOULD I DO? BCBS LA Business Associate Profile Electronic Remittance Advice (ERA) Enrollment form If you would like to receive ERAs through
AETNA BETTER HEALTH AETNA BETTER HEALTH KIDS 2000 Market Street, Suite 850 Philadelphia, PA Fax
 Instructions for Electronic Funds Transfer (EFT) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Funds Transfer (EFT) Authorization Agreement Form. Missing,
Instructions for Electronic Funds Transfer (EFT) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Funds Transfer (EFT) Authorization Agreement Form. Missing,
BLUE CROSS BLUE SHIELD LOUISIANA (53120) ERA ENROLLMENT INSTRUCTIONS
 ERA ENROLLMENT INSTRUCTIONS") BLUE CROSS BLUE SHIELD LOUISIANA (53120) ERA ENROLLMENT INSTRUCTIONS WHAT FORM(S) SHOULD I DO? Electronic Remittance Advice (ERA) Enrollment Form WHERE SHOULD I SEND THE FORM(S)? Email to: edich@bcbsla.com;
BLUE CROSS BLUE SHIELD LOUISIANA (53120) ERA ENROLLMENT INSTRUCTIONS WHAT FORM(S) SHOULD I DO? Electronic Remittance Advice (ERA) Enrollment Form WHERE SHOULD I SEND THE FORM(S)? Email to: edich@bcbsla.com;
Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
(EHR) Incentive Program
 Incentive Program") REGISTRATION USER GUIDE For Eligible Professionals Medicare Electronic Health Record (EHR) Incentive Program JULY 2012 (07.02.12 ver8) CONTENTS Step 1...Getting started 3 Step 2... Login 5 Step 3...Welcome
REGISTRATION USER GUIDE For Eligible Professionals Medicare Electronic Health Record (EHR) Incentive Program JULY 2012 (07.02.12 ver8) CONTENTS Step 1...Getting started 3 Step 2... Login 5 Step 3...Welcome
Electronic Payments & Statements (EPS) Frequently Asked Questions (FAQs)
 Frequently Asked Questions (FAQs)") Electronic Payments & Statements (EPS) Frequently Asked Questions (FAQs) As of August 25, 2014, your PAF reimbursements can be made by direct deposit. How do I enroll for direct deposit? You can enroll
Electronic Payments & Statements (EPS) Frequently Asked Questions (FAQs) As of August 25, 2014, your PAF reimbursements can be made by direct deposit. How do I enroll for direct deposit? You can enroll
AETNA BETTER HEALTH OF ILLINOIS 333 W. Wacker Drive Suite 2100, MC F646 Chicago, IL Fax
 Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
Provider Portal Claim Features Training MHO
 Provider Portal Claim Features Training MHO-2585 0119 MOLINA HEALTHCARE S PROVIDER PORTAL The Provider Portal is secure and available 24 hours a day, seven days a week. Register for access to our Provider
Provider Portal Claim Features Training MHO-2585 0119 MOLINA HEALTHCARE S PROVIDER PORTAL The Provider Portal is secure and available 24 hours a day, seven days a week. Register for access to our Provider
Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 THE 2018 HNFS ENROLLMENT IS ALSO REQUIRED WHEN FILLING THIS OUT PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to
THE 2018 HNFS ENROLLMENT IS ALSO REQUIRED WHEN FILLING THIS OUT PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to
Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
Revision History. Document Version. Date Name Comments /26/2017 Training and Development Initial Creation
 Pharmaceutical Assistance Contract for the Elderly (PACE)/ Pharmaceutical Assistance Contract for the Elderly Needs Enhancement Tier (PACENET)Web Provider Enrollment/Provider Management Corporate User
Pharmaceutical Assistance Contract for the Elderly (PACE)/ Pharmaceutical Assistance Contract for the Elderly Needs Enhancement Tier (PACENET)Web Provider Enrollment/Provider Management Corporate User
220 Burnham Street South Windsor, CT Vox Fax
 MISSISSIPPI MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER SPECIAL NOTES ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED Dual Delivery of v5010 X12 835 and Proprietary
MISSISSIPPI MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER SPECIAL NOTES ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED Dual Delivery of v5010 X12 835 and Proprietary
Overview. IHCP Provider Name and Address Maintenance. indianamedicaid.com
 Overview Form indianamedicaid.com Enrolled providers use this form to update the name and address information that is part of their Provider Profile. Four name/address types are maintained for each provider
Overview Form indianamedicaid.com Enrolled providers use this form to update the name and address information that is part of their Provider Profile. Four name/address types are maintained for each provider
AETNA BETTER HEALTH OF LOUISIANA 2400 Veterans Memorial Blvd., Suite 200 Kenner, LA Fax
 Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
PAYER ENROLLMENT INSTRUCTIONS FOR
 PAYER ENROLLMENT INSTRUCTIONS FOR Before enrolling please be sure your Revenue Performance Advisor contract includes the transactions you will be using. If you are unsure of the transactions you are contracted
PAYER ENROLLMENT INSTRUCTIONS FOR Before enrolling please be sure your Revenue Performance Advisor contract includes the transactions you will be using. If you are unsure of the transactions you are contracted
Thank you, and enjoy the webinar.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Simplify Office Administrative Tasks
 Quick Reference Guide Simplify Office Administrative Tasks Keep this Quick Reference Guide nearby to simplify pre-visit planning and post-visit tasks. Website: Patient care forms Pre-auth needed tool Superior
Quick Reference Guide Simplify Office Administrative Tasks Keep this Quick Reference Guide nearby to simplify pre-visit planning and post-visit tasks. Website: Patient care forms Pre-auth needed tool Superior
Provider Information Management System (PIMS) User Guide
 User Guide") Provider Information Management System (PIMS) User Guide v2017_1016 Overview The Provider Information Management System (PIMS) application is used to maintain provider accounts. It is accessed online from
Provider Information Management System (PIMS) User Guide v2017_1016 Overview The Provider Information Management System (PIMS) application is used to maintain provider accounts. It is accessed online from
CAQH Solutions TM EnrollHub TM Provider User Guide Chapter 3 - Create & Manage Enrollments. Table of Contents
 CAQH Solutions TM EnrollHub TM Provider User Guide Chapter 3 - Create & Manage Enrollments Table of Contents 3 CREATE & MANAGE EFT ENROLLMENTS 2 3.1 OVERVIEW OF THE EFT ENROLLMENT PROCESS 3 3.2 ADD PROVIDER
CAQH Solutions TM EnrollHub TM Provider User Guide Chapter 3 - Create & Manage Enrollments Table of Contents 3 CREATE & MANAGE EFT ENROLLMENTS 2 3.1 OVERVIEW OF THE EFT ENROLLMENT PROCESS 3 3.2 ADD PROVIDER
Oregon registration will open next Monday, the 26th. First register with CMS, then with your state.
 Sent: Tuesday, September 20, 2011 2:53 PM Subject: Meaningful Use Registration I want to make sure that the Portland Area I/T/U's are on track to receive the EHR Incentive payments. So far, who has registered
Sent: Tuesday, September 20, 2011 2:53 PM Subject: Meaningful Use Registration I want to make sure that the Portland Area I/T/U's are on track to receive the EHR Incentive payments. So far, who has registered
Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account
 PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
PAYER ID: SUBMITTER ID: 1 Provider Organization Practice/ Facility Name Change Healthcare ERA Provider Information Form *This form is to ensure accuracy in updating the appropriate account Provider Name
New York Medicaid Provider Resource Guide
 New York Medicaid Provider Resource Guide Thank you for being a star member of our provider team. WellCare Health Plans, Inc., (WellCare) understands that having access to the right tools can help you
New York Medicaid Provider Resource Guide Thank you for being a star member of our provider team. WellCare Health Plans, Inc., (WellCare) understands that having access to the right tools can help you
4350 E. Cotton Center Boulevard Building D Phoenix, AZ / Fax
 Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
IntegraFlex Employee Portal. Simplify your healthcare finances with convenience, online access to your tax-advantaged benefit account
 IntegraFlex Employee Portal Simplify your healthcare finances with convenience, online access to your tax-advantaged benefit account 1 IntegraFlex Employee Portal Contents Getting started... 2 Registration...
IntegraFlex Employee Portal Simplify your healthcare finances with convenience, online access to your tax-advantaged benefit account 1 IntegraFlex Employee Portal Contents Getting started... 2 Registration...
Medicare Enrollment Application Submission Options
 The Basics of Internet-based Provider Enrollment, Chain and Ownership System (PECOS) for Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Suppliers Beginning October 4, 2010, the
The Basics of Internet-based Provider Enrollment, Chain and Ownership System (PECOS) for Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Suppliers Beginning October 4, 2010, the
AETNA BETTER HEALTH OF OHIO 7400 W. Campus Rd. New Albany, OH Fax
 Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
icare s Provider Portal Guide
 icare s Provider Portal Guide 2 CONTENTS New Provider Registration... 4 New Registration...5 Login Page 9 Sign In 9 Forget Your Password...10 Provider Home Page 12 Track Request 12 Contact Us.. 14 Provider
icare s Provider Portal Guide 2 CONTENTS New Provider Registration... 4 New Registration...5 Login Page 9 Sign In 9 Forget Your Password...10 Provider Home Page 12 Track Request 12 Contact Us.. 14 Provider
220 Burnham Street South Windsor, CT Vox Fax
 LOUISIANA BLUE CROSS BLUE SHIELD DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 23739 SPECIAL NOTES ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CCD+ REASSOCIATION SEND
LOUISIANA BLUE CROSS BLUE SHIELD DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 23739 SPECIAL NOTES ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CCD+ REASSOCIATION SEND
Instructions for Completing the Paper Electronic Remittance Advice (ERA) Enrollment Application
 Enrollment Application") Instructions for Completing the Paper Electronic Remittance Advice (ERA) Enrollment Application General Instructions for completing the Paper ERA Enrollment Application: Please type or print legibly Complete
Instructions for Completing the Paper Electronic Remittance Advice (ERA) Enrollment Application General Instructions for completing the Paper ERA Enrollment Application: Please type or print legibly Complete
Quality Payment Program
 Guide for Obtaining a Physician Quality and Value Programs (Registration for the CMS Web Interface and/or CAHPS for MIPS Survey) Role for an Existing EIDM User I. Introduction This guide is for users who
Guide for Obtaining a Physician Quality and Value Programs (Registration for the CMS Web Interface and/or CAHPS for MIPS Survey) Role for an Existing EIDM User I. Introduction This guide is for users who
(EHR) Incentive Program
 Incentive Program") REGISTRATION USER GUIDE For Eligible Professionals Medicaid Electronic Health Record (EHR) Incentive Program DECEMBER 2010 (12.28.10 ver2) CONTENTS Step 1... Getting started 3 Step 2... Login instruction
REGISTRATION USER GUIDE For Eligible Professionals Medicaid Electronic Health Record (EHR) Incentive Program DECEMBER 2010 (12.28.10 ver2) CONTENTS Step 1... Getting started 3 Step 2... Login instruction
Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation
 Enrollment/Change/Cancellation") Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
Instructions for Electronic Remittance Advice (ERA) Enrollment/Change/Cancellation Page 1 Please use this guide to prepare/complete your Electronic Remittance Advice (ERA) Authorization Agreement Form.
220 Burnham Street South Windsor, CT Vox Fax
 220 Burnham Street South Windsor, CT 06074 Vox 888-255-7293 Fax 860-289-0055 KANSAS MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER CKKS1 SPECIAL NOTES 1. Upon
220 Burnham Street South Windsor, CT 06074 Vox 888-255-7293 Fax 860-289-0055 KANSAS MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER CKKS1 SPECIAL NOTES 1. Upon
Setting up Providers for Successful MU Attestation Part One: Steps You Need to Take with CMS
 Setting up Providers for Successful MU Attestation Part One: Steps You Need to Take with CMS Illinois EHR Incentive Help Desk muhelpdesk@chitrec.org 855-684-3571 Agenda Modify EHR Program Registration
Setting up Providers for Successful MU Attestation Part One: Steps You Need to Take with CMS Illinois EHR Incentive Help Desk muhelpdesk@chitrec.org 855-684-3571 Agenda Modify EHR Program Registration
SoonerCare Provider Information
 ATTACHMENT B-2006 SoonerCare Provider Program Information PLEASE READ THE DIRECTIONS CAREFULLY All providers must complete the Uniform Credentialing Application. It must be 100% complete, including required
ATTACHMENT B-2006 SoonerCare Provider Program Information PLEASE READ THE DIRECTIONS CAREFULLY All providers must complete the Uniform Credentialing Application. It must be 100% complete, including required
220 Burnham Street South Windsor, CT Vox Fax
 WASHINGTON BLUE CROSS BLUE SHIELD (PREMERA) DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 47570 ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CCD+ REASSOCIATION SEND
WASHINGTON BLUE CROSS BLUE SHIELD (PREMERA) DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBER 47570 ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CCD+ REASSOCIATION SEND
1304 Vermillion Street Hastings, MN Ph Fax
 Page 1 of 1 2/24/2014 NEW MEXICO MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBERS CKNM1 ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CCD+ Reassociation SEND REGISTRATION
Page 1 of 1 2/24/2014 NEW MEXICO MEDICAID DENTAL ELECTRONIC REMITTANCE ADVICE (ERA) ENROLLMENT REGISTRATION PAYER ID NUMBERS CKNM1 ELECTRONIC REGISTRATIONS AGREEMENTS REQUIRED CCD+ Reassociation SEND REGISTRATION
Revision History. Document Version. Date Name Comments
 Pharmaceutical Assistance Contract for the Elderly (PACE)/Pharmaceutical Assistance Contract for the Elderly Needs Enhancement Tier (PACENET) Web Provider Enrollment/Provider Management Independent Version
Pharmaceutical Assistance Contract for the Elderly (PACE)/Pharmaceutical Assistance Contract for the Elderly Needs Enhancement Tier (PACENET) Web Provider Enrollment/Provider Management Independent Version
EDI Electronic Funds Transfer (EFT) and Electronic Remittance Advice (ERA) Online Enrollment Instructions
 and Electronic Remittance Advice (ERA) Online Enrollment Instructions") Welcome to the instructions for online enrollment for your EFA and EFT. Please follow the instructions below to improve your experience in enrolling and receiving your electronic transactions. If at any
Welcome to the instructions for online enrollment for your EFA and EFT. Please follow the instructions below to improve your experience in enrolling and receiving your electronic transactions. If at any
Infinedi, LLC. Frequently Asked Questions
 Infinedi, LLC Frequently Asked Questions Who are we? Infinedi has been helping medical providers better manage their practices since 1986 by providing the finest EDI services available. Infinedi is a privately
Infinedi, LLC Frequently Asked Questions Who are we? Infinedi has been helping medical providers better manage their practices since 1986 by providing the finest EDI services available. Infinedi is a privately
Nebraska Provider Screening and Enrollment New Group Member New Group Member Profile
 Nebraska Provider Screening and Enrollment New Group Member New Group Member Profile The steps below will guide you through filling out or updating a Group Member Profile. All applications must be submitted
Nebraska Provider Screening and Enrollment New Group Member New Group Member Profile The steps below will guide you through filling out or updating a Group Member Profile. All applications must be submitted
MEDICAID FLORIDA ELECTRONIC REMITTANCE ADVICE ENROLLMENT INSTRUCTIONS 77027
 MEDICAID FLORIDA ELECTRONIC REMITTANCE ADVICE ENROLLMENT INSTRUCTIONS 77027 HOW LONG DOES PRE-ENROLLMENT TAKE? Please allow 3 weeks for processing. HOW DO I ENROLL / WHAT FORM(S) SHOULD I DO? Option 1:
MEDICAID FLORIDA ELECTRONIC REMITTANCE ADVICE ENROLLMENT INSTRUCTIONS 77027 HOW LONG DOES PRE-ENROLLMENT TAKE? Please allow 3 weeks for processing. HOW DO I ENROLL / WHAT FORM(S) SHOULD I DO? Option 1:
Agent appointment and credentialing quick reference guide
 Questions? Email us at brokers@brighthealthplan.com or call us at 1-888-325-1747 Monday-Friday 8:30am 5pm (CST) Agent appointment and credentialing quick reference guide Welcome to the Bright Health appointment
Questions? Email us at brokers@brighthealthplan.com or call us at 1-888-325-1747 Monday-Friday 8:30am 5pm (CST) Agent appointment and credentialing quick reference guide Welcome to the Bright Health appointment
MISSISSIPPI MEDICAID ERA CONTRACT INSTRUCTIONS (SKMS0)
") MISSISSIPPI MEDICAID ERA CONTRACT INSTRUCTIONS (SKMS0) An original signature is required. Please MAIL all pages of your completed and signed forms to: ABILITY ATTN: Enrollment One MetroCenter 4010 W. Boy
MISSISSIPPI MEDICAID ERA CONTRACT INSTRUCTIONS (SKMS0) An original signature is required. Please MAIL all pages of your completed and signed forms to: ABILITY ATTN: Enrollment One MetroCenter 4010 W. Boy
Quality Payment Program
 Guide for Obtaining a New EIDM Account with a Physician Quality and Value Programs (Registration for the CMS Web Interface and/or CAHPS for MIPS Survey) Role I. Introduction This guide is for users who
Guide for Obtaining a New EIDM Account with a Physician Quality and Value Programs (Registration for the CMS Web Interface and/or CAHPS for MIPS Survey) Role I. Introduction This guide is for users who
1. Go to https://providernet.adminisource.com. 2. Click the Register button. 3. Accept the Terms and Conditions
 Page 1 of 12 Change Healthcare ProviderNet Registration 1. Go to https://providernet.adminisource.com 2. Click the Register button 3. Accept the Terms and Conditions Page 2 of 12 4. Enter provider verification
Page 1 of 12 Change Healthcare ProviderNet Registration 1. Go to https://providernet.adminisource.com 2. Click the Register button 3. Accept the Terms and Conditions Page 2 of 12 4. Enter provider verification
BHSDSTAR. User Guide-Vendor Registration. Updated 3/31/17. Vendor Registration User Guide Version 1.0. BHSD User Guide Page 1 of 11
 User Guide-Vendor Registration Updated 3/31/17 BHSD User Guide Page 1 of 11 Table of Contents 1. Purpose and Introduction... 3 1.1 General Information... 3 1.2 Vendor Registration Process Overview... 3
User Guide-Vendor Registration Updated 3/31/17 BHSD User Guide Page 1 of 11 Table of Contents 1. Purpose and Introduction... 3 1.1 General Information... 3 1.2 Vendor Registration Process Overview... 3
Provider Secure Portal User Manual
 Provider Secure Portal User Manual Copyright 2011 Centene Corporation. All rights reserved. Operational Training 2 August 2011 Table of Contents Provider Secure Portal... 5 Registration... 6 Provider -
Provider Secure Portal User Manual Copyright 2011 Centene Corporation. All rights reserved. Operational Training 2 August 2011 Table of Contents Provider Secure Portal... 5 Registration... 6 Provider -
SECURE PROVIDER WEB PORTAL AND ELECTRONIC CLAIMS SUBMISSION SERVICE
 SECURE PROVIDER WEB PORTAL AND ELECTRONIC CLAIMS SUBMISSION SERVICE SECURE PROVIDER WEB PORTAL AND ELECTRONIC CLAIMS SUBMISSION SERVICE INTRODUCTION...3 COMPUTER AND INTERNET REQUIREMENTS...4 REGISTERING
SECURE PROVIDER WEB PORTAL AND ELECTRONIC CLAIMS SUBMISSION SERVICE SECURE PROVIDER WEB PORTAL AND ELECTRONIC CLAIMS SUBMISSION SERVICE INTRODUCTION...3 COMPUTER AND INTERNET REQUIREMENTS...4 REGISTERING
MEDICAID PENNSYLVANIA ERA ENROLLMENT INSTRUCTIONS - MCDPA
 MEDICAID PENNSYLVANIA ERA ENROLLMENT INSTRUCTIONS - MCDPA HOW LONG DOES PRE-ENROLLMENT TAKE? Please allow four (4) weeks for the enrollment application process. If after five (5) weeks you do not start
MEDICAID PENNSYLVANIA ERA ENROLLMENT INSTRUCTIONS - MCDPA HOW LONG DOES PRE-ENROLLMENT TAKE? Please allow four (4) weeks for the enrollment application process. If after five (5) weeks you do not start
This bulletin provides additional information about the change in First Steps (FS) processors as outlined in BT dated February 3, 2006.
 processors as outlined in BT dated February 3, 2006.") INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 6 1 0 A P R I L 2 0, 2 0 0 6 To: First Steps Providers Subject: First Steps Update Information Overview This bulletin provides
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 6 1 0 A P R I L 2 0, 2 0 0 6 To: First Steps Providers Subject: First Steps Update Information Overview This bulletin provides
Link 1500 / Online Claims Entry User Guide
 Link 1500 / Online Claims Entry User Guide ABILITY Network Inc Copyright and Trademark Copyright Copyright 2016 ABILITY Network Inc. All Rights Reserved. All text, images, and graphics, and other materials
Link 1500 / Online Claims Entry User Guide ABILITY Network Inc Copyright and Trademark Copyright Copyright 2016 ABILITY Network Inc. All Rights Reserved. All text, images, and graphics, and other materials
Part B. NGSConnex User Guide. https:/www.ngsconnex.com. Visit our YouTube Channel to view all of our videos! https://www.youtube.com/user/ngsmedicare
 NGSConnex User Guide Part B This guide provides information for our Part B providers on the different options available within our self-service portal, NGSConnex. https:/www.ngsconnex.com Visit our YouTube
NGSConnex User Guide Part B This guide provides information for our Part B providers on the different options available within our self-service portal, NGSConnex. https:/www.ngsconnex.com Visit our YouTube
BBP Admin Participant Portal. Simplify your healthcare finances with convenient, online access to your tax-advantaged benefit account
 BBP Admin Participant Portal Simplify your healthcare finances with convenient, online access to your tax-advantaged benefit account 1 BBP Admin Participant Portal Contents Getting started... 2 Registration...
BBP Admin Participant Portal Simplify your healthcare finances with convenient, online access to your tax-advantaged benefit account 1 BBP Admin Participant Portal Contents Getting started... 2 Registration...
MASSACHUSETTS MEDICAID EDI CONTRACT INSTRUCTIONS (SKMA0)
") MASSACHUSETTS MEDICAID EDI CONTRACT INSTRUCTIONS (SKMA0) Submit the completed Contract Setup Form to: ABILITY Network, ATTN: Enrollment FAX: 888.837.2232 EMAIL: setup@abilitynetwork.com INSTRUCTIONS Print
MASSACHUSETTS MEDICAID EDI CONTRACT INSTRUCTIONS (SKMA0) Submit the completed Contract Setup Form to: ABILITY Network, ATTN: Enrollment FAX: 888.837.2232 EMAIL: setup@abilitynetwork.com INSTRUCTIONS Print
Provider Portal. User Manual. Therapists and Health Practitioners
 Provider Portal User Manual Therapists and Health Practitioners Table of Contents 1. Introduction... 3 2. Registering for the Provider Portal... 4 i. Changing Your Password...6 ii. Accepting Terms and
Provider Portal User Manual Therapists and Health Practitioners Table of Contents 1. Introduction... 3 2. Registering for the Provider Portal... 4 i. Changing Your Password...6 ii. Accepting Terms and
Electronic Transaction Registration Packet
 Electronic Transaction Registration Packet Wellmark Blue Cross and Blue Shield of Iowa and Wellmark Blue Cross and Blue Shield of South Dakota are Independent Licensees of the Blue Cross and Blue Shield
Electronic Transaction Registration Packet Wellmark Blue Cross and Blue Shield of Iowa and Wellmark Blue Cross and Blue Shield of South Dakota are Independent Licensees of the Blue Cross and Blue Shield
Online Banking Wire Transfer Enrollment
 Online Banking Wire Transfer Enrollment Revised 9/2016 Page 1 Overview Wire Transfers (also referred to as Wire Transfer Payments) are a trusted instrument for transferring funds quickly and conveniently
Online Banking Wire Transfer Enrollment Revised 9/2016 Page 1 Overview Wire Transfers (also referred to as Wire Transfer Payments) are a trusted instrument for transferring funds quickly and conveniently
QuickClaim Guide Group Health Cooperative of Eau Claire GHC13009
 QuickClaim Guide Administered by: Group Health Cooperative of Eau Claire 2503 North Hillcrest Parkway Altoona, WI 54720 715.552.4300 or 888.203.7770 group-health.com 2013 Group Health Cooperative of Eau
QuickClaim Guide Administered by: Group Health Cooperative of Eau Claire 2503 North Hillcrest Parkway Altoona, WI 54720 715.552.4300 or 888.203.7770 group-health.com 2013 Group Health Cooperative of Eau
HEALTHCOMP (85729) ERA ENROLLMENT INSTRUCTIONS
 ERA ENROLLMENT INSTRUCTIONS") HEALTHCOMP (85729) ERA ENROLLMENT INSTRUCTIONS WHAT FORM(S) SHOULD I DO? Electronic Remittance Advice (ERA) Authorization Agreement Electronic Funds Transfer (EFT) Authorization Agreement WHERE SHOULD
HEALTHCOMP (85729) ERA ENROLLMENT INSTRUCTIONS WHAT FORM(S) SHOULD I DO? Electronic Remittance Advice (ERA) Authorization Agreement Electronic Funds Transfer (EFT) Authorization Agreement WHERE SHOULD
My SmartCare Online Portal
 My SmartCare Online Portal Your reimbursement management portal from Benefit Coordinators Corporation (BCC). Customer Service Call Center: 800-685-6100 M-Thurs: 8:00am - 8:00pm ET / F: 8:00am - 6:00pm
My SmartCare Online Portal Your reimbursement management portal from Benefit Coordinators Corporation (BCC). Customer Service Call Center: 800-685-6100 M-Thurs: 8:00am - 8:00pm ET / F: 8:00am - 6:00pm
Commonwealth of Kentucky KY Medicaid KyHealth Net Long Term Care (LTC) Companion Guide
 Companion Guide") Commonwealth of Kentucky KY Medicaid KyHealth Net Long Term Care (LTC) Companion Guide Version 3.2 March 21, 2017 Revision History Document Version Date Name Comments 1.0 04/27/2010 EDI Created. 1.1 06/8/2010
Commonwealth of Kentucky KY Medicaid KyHealth Net Long Term Care (LTC) Companion Guide Version 3.2 March 21, 2017 Revision History Document Version Date Name Comments 1.0 04/27/2010 EDI Created. 1.1 06/8/2010